iPharma Pharmacy's Low Libido Products!
- Thank you for showing interest in our low-libido products
- Please complete the secure form below to receive your prescription (treatment will depend on your eligibility)
- A member of our staff will contact you within 24HR

Erectile Dysfunction and Low Libido
Consult with Our Pharmacist for a Prescription to Address Erectile Dysfunction for Men and Low Libido for Women.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for treating erectile dysfunction in a single visit.
$20 Per Consultation.

Viagra Troche
Transfer your prescription to us and receive a FREE VIAGRA troche sample!
Clinical Services
iPharma Pharmacy, in collaboration with Scripted, is your neighborhood pharmacy committed to saving you both time and money.

Services we offer!
We’re thrilled to offer a range of clinical services, which traditionally necessitated a doctor’s visit, directly at our pharmacy.
Click the ‘Schedule Appointment’ button below each service to view more details and arrange your appointment.
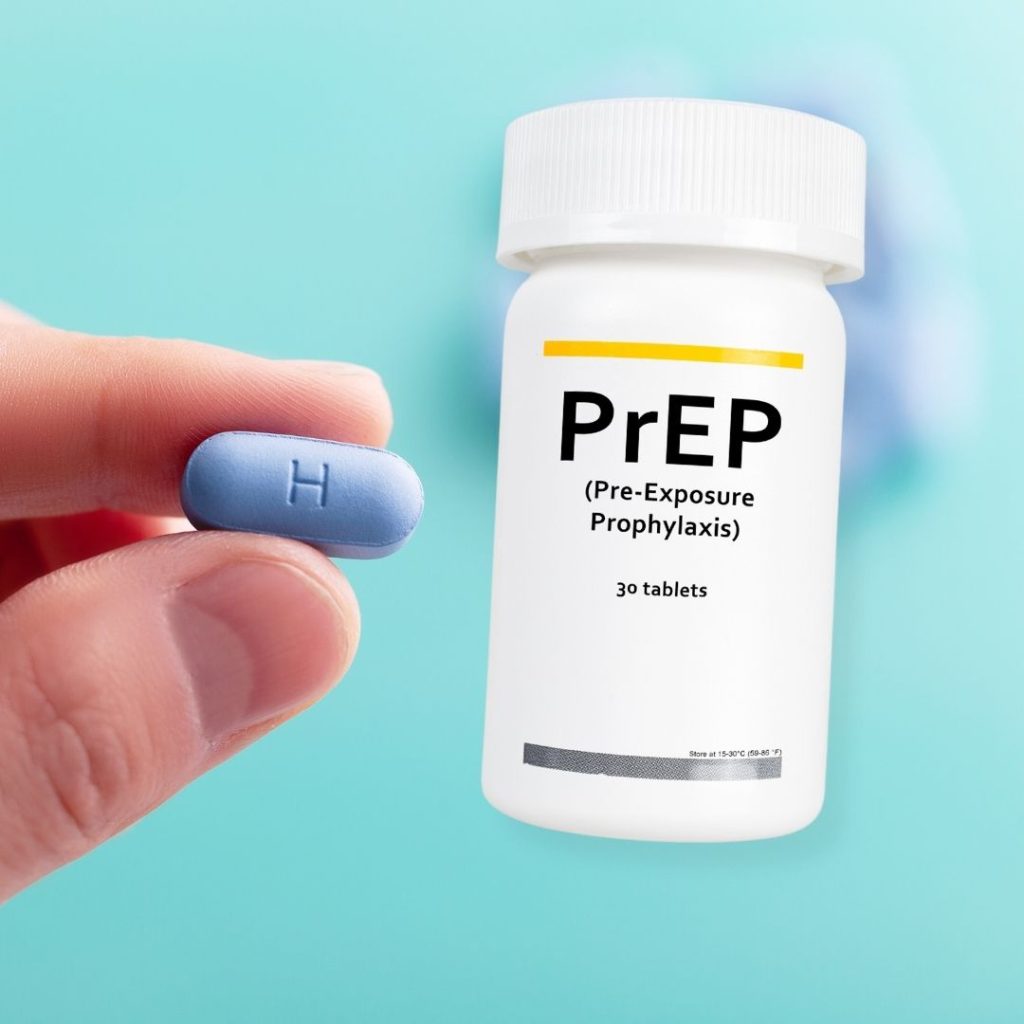

PrEP HIV Treatment
iPharma Pharmacy now offers PrEP prescriptions. Consult with our pharmacists to obtain a fresh prescription for PrEP as a preventive measure against HIV.
Discuss your medical background with our pharmacist and get both a prescription and PrEP medication in a single appointment.
$20 Per Consultation.
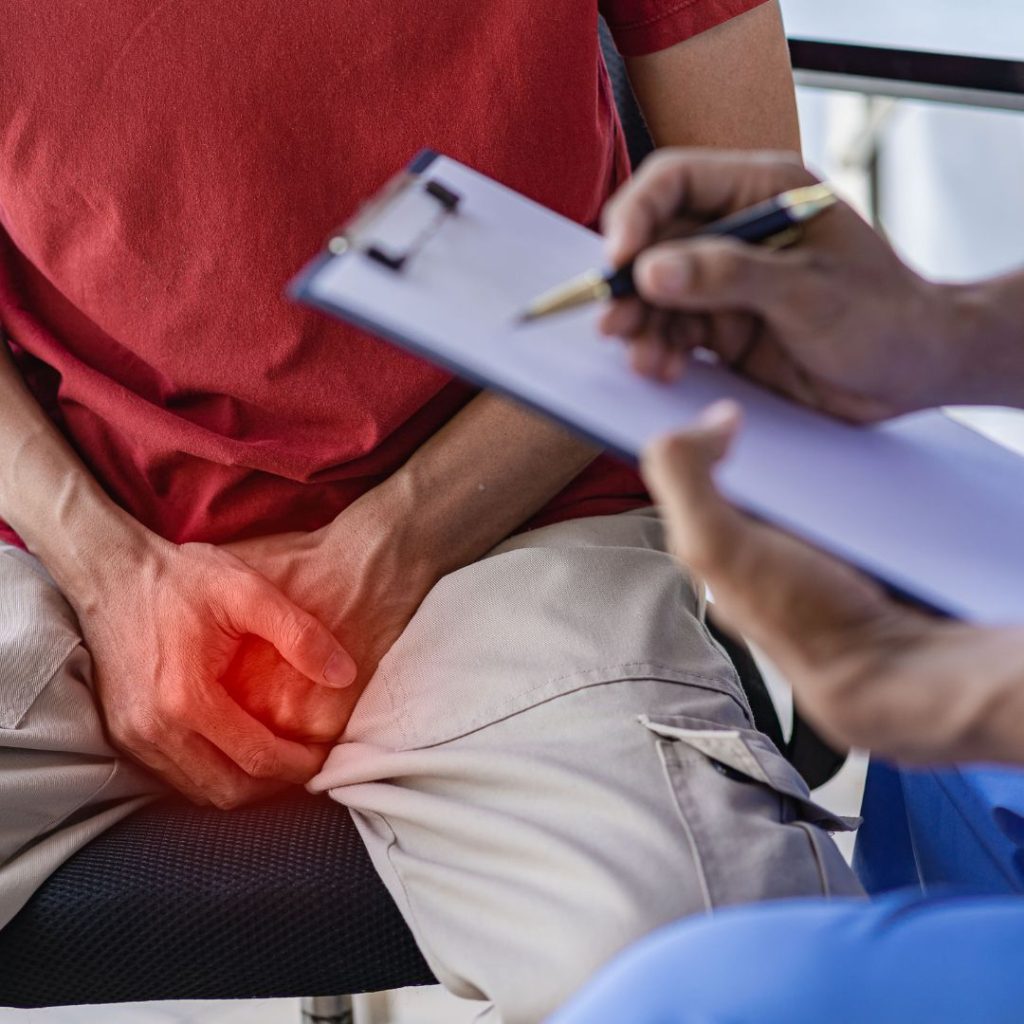
Erectile Dysfunction Diagnosis and Treatment
Consult with Our Pharmacist for a Prescription to Address Erectile Dysfunction
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for treating erectile dysfunction in a single visit.
$0 Per Consultation.
Hair Loss Prevention
Speak with Our Pharmacist for a Prescription Tailored for Hair Loss Prevention
Discuss your symptoms and health background with our pharmacist to secure a prescription and medication to prevent hair loss, all within one appointment.
$20 Per Consultation.



Hormonal Birth Control Assessment and Treatment:
Consult with Our Pharmacist for an Oral Birth Control Prescription.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for hormonal birth control in a single visit.
$20 Per Consultation.
Emergency Contraception:
Consult with Our Pharmacist for an Emergency Birth Control (Plan B) Prescription.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for emergency contraception in a single visit.
$0 Per Consultation.
Anaphylaxis Autoinjector (EpiPen):
Consult with Our Pharmacist for an EpiPen Prescription to Prevent an Anaphylactic Reaction.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and an anaphylaxis autoinjector in a single visit.
$20 Per Consultation.



UTI Diagnosis and Treatment
Receive an evaluation from our pharmacist and obtain a prescription to address a straightforward UTI.
Discuss your symptoms and medical history with our pharmacists to secure both a prescription and the medication needed to manage an uncomplicated UTI in a single visit.
$20 Per Consultation
Cold Sore Diagnosis and Treatment
Consult with Our Pharmacist for a Prescription to Address Mild Cough.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for treating mild Cough in a single visit.
$20 Per Consultation.
Mild Acne Diagnosis and Treatment
Secure an Acne Treatment Prescription from Our Pharmacist
Discuss your symptoms and medical history with our pharmacist to obtain a prescription and medication for mild acne treatment in a single visit.
$20 Per Consultation.



Allergic Rhinitis:
Consult with Our Pharmacist for a Prescription to address Allergic Rhinitis.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for treating allergic rhinitis in a single visit.
$20 Per Consultation.
Motion Sickness:
Consult with Our Pharmacist for a Prescription to Address Motion Sickness.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for treating motion sickness in a single visit.
$20 Per Consultation.
Naloxone:
Consult with Our Pharmacist for a Prescription for Naloxone as a Preventative Measure Against Opioid Overdose.
Explore your symptoms and medical history with our pharmacist to obtain a prescription and medication for Naloxone in a single visit.
$0 Per Consultation.

PeP:
iPharma Pharmacy now offers PeP prescriptions. Consult with our pharmacists to obtain a fresh prescription for PeP within 72 hours of a possible exposure to HIV to prevent HIV infection.
Discuss your medical background with our pharmacist and get both a prescription and PeP medication in a single appointment.
$20 Per Consultation.
This Can Be Secondary Heading. (needs adjustment)
Address
Riverside Building, County Hall, South Bank, London SE1 7PB, United Kingdom
Hours
- Weekdays - 8AM to 5PM
- Saturday - 11AM to 4PM
- Sunday - Holiday